Introduction
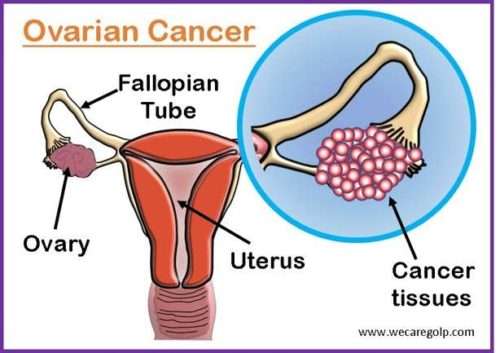
Ovarian cancer is cancer that originates in the tissues of the ovary, the primary sex organ of females that produces female hormones and eggs for reproduction. Among all the female reproductive cancers, ovarian cancer is the most fatal. Therefore, it is a matter of global concern as it is typically diagnosed at a late stage and has no effective screening strategy.
Anatomy of Ovary
- Ovaries are the paired reproductive glands responsible to produce ova (eggs) and sex hormones.
- They are located on either side of the uterus within the broad ligament below the fallopian tubes.
- The ovaries are covered on the outside by germinal epithelium made of a layer of simple cuboidal epithelium.
- Underneath the germinal epithelium, the dense connective tissue is found which can further be divided into n outer cortex and inner medulla.
Cortex
- The ovarian cortex is made of connective tissue.
- It appears denser and more granular.
- It includes all the ovarian follicles at various stages of development and degeneration in the cortex.
Medulla
- It consists of loose connective tissue with abundant blood vessels, lymphatic vessels, and nerve fibers.
Incidence
- Ovarian cancer is the eighth most diagnosed and seventh most lethal cancer among women worldwide.
- Globally, 225,500 new cases are diagnosed every year, with 140,200 cancer-specific deaths.
- Epithelial ovarian cancer is the fourth most common female cancer-causing death in the developed world.
- The approximate lifetime risk of developing ovarian cancer is about one in 60 in the UK.
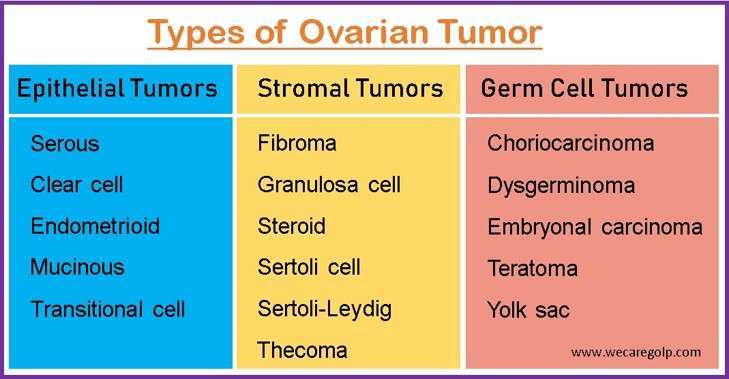
Types of Ovarian Tumor
Depending on the variable identifiable risk factors, cells of origin, and molecular compositions, the ovarian tumor can be divided into different histological subtypes. Ovarian tumors may be benign (non-cancerous), borderline (low-malignant potential, or malignant (cancerous). Benign tumors never spread. On the other hand, cancerous tumors can metastasize to other parts of the body and may cause death.
Epithelial tumors
- It is originated in the thin layer of tissue that covers the outside of the ovaries.
- Almost all (90%) of ovarian cancers are epithelial tumors. High-grade serous carcinomas make up most ovarian cancers.
Stromal tumors
- It originates in the ovarian tissue that contains hormone-producing cells.
Germ cell tumors
- It is rare and originates in egg-producing cells.
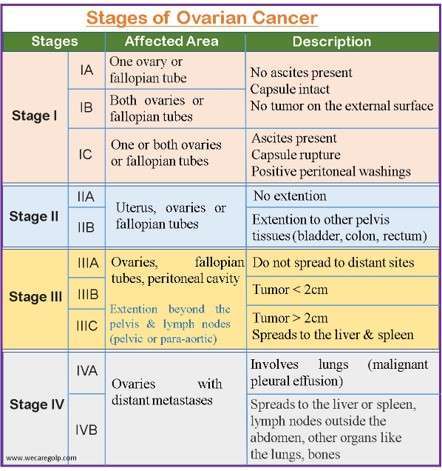
Stages of Ovarian Cancer
- The stage of ovarian cancer identifies the extent of disease present at the time of diagnosis.
- Accurate staging of ovarian cancer is important for the provision of individualized care and management.
- The following figure shows the four stages according to the International Federation of Gynecology and Obstetrics (FIGO).
Causes of Ovarian Cancer
- The actual cause is not clear.
- When cells have DNA changes (mutation) in or near the ovaries, it may develop.
- The DNA mutation instructs the cells to rapidly expand and multiply, resulting in a tumor of cancer cells.
- When healthy cells would die, the cancer cells continue to live. They can spread (metastasize) to other parts of the body by invading nearby tissues.
Risk factors of Ovarian Cancer
- Genetics
- Inheritance of mutant genes BRCA 1 and BRCA 2 (breast cancer susceptibility genes)
- Hereditary non-polyposis colorectal cancer syndrome (HNPCC), also known as Lynch syndrome
- Family history of ovarian cancer
- Reproductive factors
- Nulliparity
- First child after the age of 35 years
- Late menopause and early menarche
- Patients with prolonged or uninterrupted ovulation
- Endometriosis
- Increasing age
- Obesity
- Smoking
- Use of anti-infertility drugs
Sign and Symptoms of Ovarian Cancer
The early stages are not associated with clinical symptoms; thus, the diagnosis of it is often delayed. However, the symptoms are persistent and gradually worsen over time. The following signs and symptoms are observed in ovarian cancer:
- Abdominal fullness or discomfort
- Bloating
- Nausea
- Indigestion
- Fatigue
- Back pain
- Pain during sex
- Urinary urgency
- A frequent need to urinate
- Back pain
- Changes in bowel patterns
- Fatigue
- Weight loss
- Discomfort in the pelvic area
In the later stages, the following signs and symptoms may be found:
- Palpable pelvic mass
- Ascites
- Diminished breath sounds
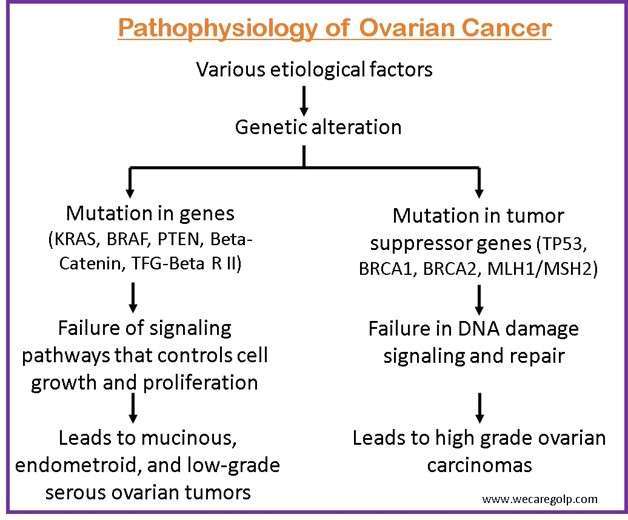
Pathophysiology of Ovarian Cancer
Diagnosis of Ovarian Cancer
History taking
- Family history of ovarian and breast cancers
- Genetic risk assessment
Physical examination
- Bimanual or pelvic examination (to check enlarged ovary or ascites)
- Rectal examination
Blood tests
- Complete blood count
- Liver function test
- Kidney function test
- Serum calcium
- Serum CA-125 (tumor marker)
Imaging tests
- Ultrasonography (USG)
- Transvaginal USG
- Abdominal USG
- Pelvic USG
- Pelvis CT scan
- Pelvis MRI
- Positron emission tomography (PET) scan
- X-rays
Other tests
- Laparoscopy
- Laparotomy
- Colonoscopy
- Needle biopsy (take a fluid sample)
Screening
- Unlike cervical cancers, ovarian cancer does not have a detectable pre-invasive phase. So, effective screening strategies for early detection of ovarian cancer do not exist.
- Screening is recommended in women with:
- Strong suspicion of ovarian cancer based on the clinical features/pelvic mass.
- Family history associated with a risk of BRCA mutation (BRCA1 or BRCA2) or other genes associated with ovarian cancer should be identified.
- However, the American College of Obstetricians and Gynecology (ACOG), U.S. Preventive Service Task Force (USPSTF), and Society of Gynecologic Oncology recommend against screening for ovarian cancer in asymptomatic women at average risk and low-risk women with cancer antigen (CA-125) or ultrasound for ovarian cancer.
Management of Ovarian Cancer
Surgical Management
Most ovarian cancers can only be treated with surgery. Initial surgical therapy includes three main objectives:
- Staging
- Cytoreduction
- Determining a definitive histologic diagnosis
Surgery for Early Disease
- Early disease refers to the malignancy confined to the ovaries (FIGO Stage I).
- Fertility-preserved surgeries are considered in young women with stage I or a tumor that is borderline or has low malignant potential.
- Surgeries for the early disease involve:
- Total abdominal hysterectomy
- Bilateral salpingo-oophorectomy
Surgery for Advanced Disease
- Advanced disease refers to ovarian cancer with metastasis to other pelvic organs.
- It involves cytoreductive surgery followed by chemotherapy.
- Neoadjuvant therapy is used along with the surgery.
- Neoadjuvant therapy is the reduction of the tumor burden before the surgery to decompress the size of the tumor.
- It may be:
- Primary surgery: It is the surgery performed for the first time, either before or after chemotherapy.
- Secondary surgery: It is the surgery performed after the primary surgery.
- Surgeries that are commonly used for the treatment and management are:
- Ovariectomy
- Adnexectomy
- Unilateral/bilateral salpingo-oophorectomy
- Debulking surgery
- Hysterectomy
- Debulking surgery is done for the residual tumor nodules less than 1 cm in maximum diameter/thickness.
Chemotherapy
- Chemotherapy refers to the use of one or more cytotoxic drugs that impair the mitosis (cell division) effectively targeting tumor cells that divide rapidly.
- Chemotherapy can be used either with surgery or on its own.
- It can be given :
- To treat cancer diseases that cannot be surgically removed
- Before surgery: to shrink cancer to boost the effectiveness of the surgery (neo-adjuvant chemotherapy)
- After surgery: to lessen the likelihood of a cancer recurrence (adjuvant chemotherapy)
- Usually used chemotherapy drugs are
- Platinum-based agent (Carboplatin, Paclitaxel): first-line drug
- Cisplatin
- Docetaxel
- Topotecan
Other Therapy Options
Immunotherapy
- Immunotherapy is used to encourage the patient’s own immune system to find and kill cancer cells.
- Immunotherapy with immune checkpoint inhibitors (ICIs) is used with a combination of chemotherapy and other cancer drugs in advanced diseases.
- Immunotherapy alone is less responsive than the combined formed.
Targeted therapy
Anti-angiogenic Inhibitor
- It stops the cancer cell from forming new blood vessels.
- The mechanism of these drugs is to stop the oxygen and food supply so that cancer cells starve and are unable to grow.
- It is generally utilized for patients with advanced ovarian cancer as a support medication to prevent or postpone malignant growth’s return.
- An example of it is Bevacizumab (Avastin).
Poly (ADP)-ribose polymerase (PARP) Inhibitor
- PARP proteins help in the self-regeneration of the cells once they are damaged.
- Thus, PARP inhibitors stop the process of regeneration in the cancer cells, prohibiting growth and larger tumor formation.
- Currently available three PARP inhibitors are
- Olaparib
- Rucaparib
- Niraparib
Hormone therapy
- Estrogen, a female hormone, is necessary for the growth of some ovarian cancers.
- The purpose of hormone therapy is to block the proliferation of cancer cells by
- Stopping estrogen production or
- Preventing already existing estrogen from getting to the cancer cells.
- The use of this therapy is usually rare.
- The available hormone therapies are
- Luteinizing-hormone-releasing hormone (LHRH) agonists: Goserelin (Zoladex) and Leuprolide (Lupron)
- Tamoxifen: Nolvadex
- Aromatase inhibitors: Letrozole (Femara), Anastrozole (Arimidex), and Exemestane (Aromasin)
Radiotherapy
Radiation therapy kills cancer cells with high-energy rays. It is performed to
- Manage advanced stages if other treatment options did not help
- Subside the symptoms like pain, discomfort, and bleeding.
Complications of Ovarian Cancer
- Infections
- Vaginal bleeding
- Edema of the extremities
- Anemia
- Bowel obstruction
- Perforation of the colon
- Urinary retention
- Pleural effusion
- Bone pain
Prevention of Ovarian Cancer
- Maintaining parity (giving birth to babies)
- Breastfeeding
- Use of oral contraceptives
- Regular exercise
- Healthy dietary habits
- Cessation of smoking habits and tobacco use
- Tubal ligation
- Hysterectomy
- Bilateral oophorectomy
Prognosis
- The important prognostic factor is the early diagnosis when tumors are small and still confined within the ovaries.
- However, the disease is not commonly recognized until an advanced stage, leading to increased mortality and morbidity.
- According to the recent research studies conducted, the median survival of ovarian cancer when treated is 40-50% at 10 years with stage-related survival for stages I, II, III, and IV of 73-92%, 45-55%, 21% and <6% respectively.
- The US Surveillance, Epidemiology, and End Results database reports that overall survival for all patients with ovarian cancer is 45.6%, with a wide variation depending on the stage of ovarian cancer.
- The 5- year survival rate in patients with stage I epithelial cancer is 92.1%, whereas the survival rate is only up to 28% for patients with advanced-stage tumors.
Summary
- Ovarian cancer is the abnormal proliferation of cells originating from the ovary.
- It is the most fatal of all female reproductive cancers.
- Currently, there is no effective screening test for ovarian cancer with diagnosis often at late stages.
- The treatment and management involve surgery, chemotherapy along with other treatment modalities.
- It remains asymptomatic until the advanced stages leading to increased mortality and morbidity. So, preventive measures should be reinforced.
References
- Mutch, D. G. (2002). Surgical management of ovarian cancer. Seminars in Oncology, 29(1), 3-8. doi:10.1053/sonc.2002.31589
- Rooth, C. (2013). Ovarian cancer: risk factors, treatment, and management. British Journal of Nursing, 22(Sup 17), S23-S30. doi: 10.12968/bjon.2013.22.sup17
- Stewart, C., Ralyea, C., & Lockwood, S. (2019). Ovarian Cancer: An Integrated Review. Seminars in Oncology Nursing, 35(2), 151-156. https://doi.org/10.1016/j.soncn.2019.02.001
- Jelovac, D., & Armstrong, D. K. (2011). Recent progress in the diagnosis and treatment of ovarian cancer. CA. A Cancer Journal for Clinicians, 61(3), 183-203. doi: 10.3322/caac.20113
- Lim, D., & Olivia, E. (2013). Precursors and pathogenesis of ovarian carcinoma. Pathology, 45(3), 229-242. doi: 10.1097/pat.0b013e32835f2264
- Alison, M. K., & Ronny, d. (2010). Ovarian Cancer Pathogenesis: A Model in Evolution, Journal of Oncology, 2010(Article ID 932371), 13 pages. https://doi.org/10.1155/2010/932371