Introduction
As the effectiveness of hemodialysis depends on the urea value, let´s first understand urea.
- Since urea has a low molecular mass (60 Dalton), it quickly indicates as a model substance for determining the dialysis dose. But urea itself has no toxic effects.
- Urea eliminates by glomerular filtration via the kidneys.
- Urea is the end product of protein metabolism in the liver. The urea level depends on function of the liver on the one hand and the nutrition on the other.
- A low predialytic urea level is therefore considered a marker of malnutrition.
- In addition, urea is not very protein-bound. Therefore, it is easily dialysable.
- However, the sole determination of the urea value before dialysis is unsuitable for assessing the dialysis quality.
- An elevated pre-dialysis urea level does not necessarily indicate poor dialysis therapy. The patient may be in good general and nutritional condition.
- Conversely, low pre-dialysis urea levels are associated with increased mortality in affected patients. It could be an indication of malnutrition.
- However, the indicators or sure signs of adequate dialysis are no blood pressure issues, no renal anemia, controlled hyperparathyroidism, and good nutritional status.
Each dialysis facility must record and report the so-called quality indicators of every patient quarterly. These include:
- Dialysis frequency: ≥ 3×/week
- Effective dialysis time: ≥ 240 min
- Kt/V: ≥ 1.2
- Hb or Hct: ≥ 10g/dl or 30%
Measurement of the Effectiveness of Hemodialysis
There are mainly two ways to measure the effectiveness of hemodialysis.
- The Urea Reduction Rate (URR)
- Kt/V
The Urea Reduction Rate (URR)
- The urea reduction rate is one type of quality measurement of the dialysis, which calculates from the urea value before and after the dialysis.
- The URR should be at least 65%, preferably 70%.
- However, many factors could determine the URR in every individual, for example, ultrafiltration, dialysis time, filter size, and regeneration of urea during dialysis.
- To calculate the URR, use following formula.

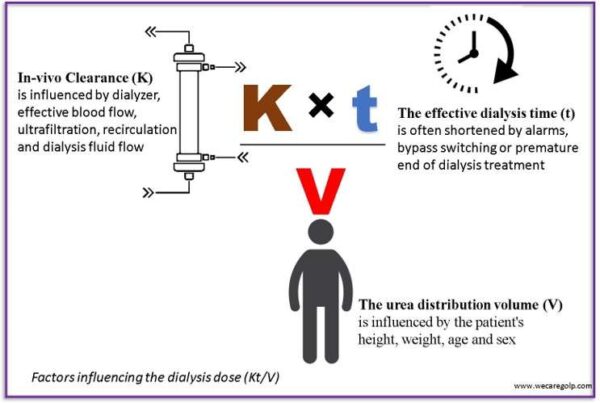
K×t/V
- Kt/V is another way to measure the effectiveness of hemodialysis.
- This parameter determines urea elimination depending on the individual patient’s specific body volume.
- However, calculating Kt/V on a rough basis does not meet the requirements.
- Option available with modern dialysis machines to measure Kt/V online during dialysis (e.g., OCM module from the company FMC), although helpful for orientation, is also insufficient.
- Not only the changing volume due to ultrafiltration and urea regeneration during dialysis but also a possible residual function of the patient’s kidneys can affect the Kt/V value.
- Here:
- K: (in ml/min) for the urea clearance of the dialyzer
- t: (in min) for the dialysis time and
- V: (in ml) for the urea distribution volume in the body.
K (Dialyzer Urea Clearance)
- The type and surface area (size) of a dialyzer, the blood pump speed, ultrafiltration, dialysate flow and possible recirculation during dialysis significantly influence the urea clearance of the dialyzer.
- A specific substance is cleared completely (after dialyzer passage) at a defined blood pump speed or with defined blood volume in a minute.
- The in vitro clearance values of all the substances are given in the product description of the dialyzers.
t (Effective Dialysis Time)
- The dialysis time can differentiate according to the patient´s health condition (3 – 5 hours). The nephrologist fixes the dialysis time as per need.
- The various factors affect the treatment time. For example, machine alarms occur during treatment, dialysis machine bypasses, and premature termination of dialysis treatment.
- Some dialysis machines can extend the treatment time after disturbances accordingly.
- Nevertheless, dialysis time is the parameter that can determine most easily with high accuracy.
V (Urea Distribution Volume)
- The urea distribution volume corresponds approximately to the total body water volume. It can roughly estimate 55% and 60% of body weight in women and men, respectively.
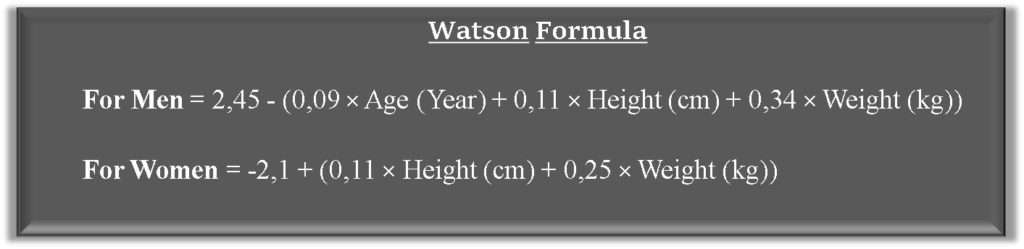
- The Watson formula calculates the V of the patient depending on the weight, height, age, and gender of the patient.
- Another way to determine urea distribution volumes is bioimpedance measuring device (e.g., BCM from Fresenius Medical Care) to determine the V. However, the expectation of the accuracy from this method is only +/- 10%.

What must be considered to optimize the Kt/V?
- A sufficiently long dialysis time
- Large dialyzer surface
- As high blood pump speed as possible
- Increasing the dialysate flow
- Large distance between fistula puncture sites and large dialysis needles
Blood Sample Collection
Pre-Dialytic Blood Collection
- Pre-dialytic blood collection must be performed from the arterial cannula immediately before dialysis before saline or heparin has been applied to avoid dilution effects.
- When using a central venous catheter, the first 10ml of blood should discard.
Post-Dialytic Blood Collection
Post-dialytic blood sampling should be performed according to the KDOQI guidelines using the “slow-flow/stop pump method”.
- Before the end of dialysis, ultrafiltration and dialysate flow shall be turned off or reduced as much as possible.
- Blood flow should reduce to 50 – 100 ml/min to minimize fistula recirculation.
- After approximately 20 seconds (15 – 30 seconds), a blood sample draws from the arterial cannula (either the blood pump is running or stops) within 15 – 30 seconds.
- In the case of a central venous catheter, 10-30 ml of blood is taken directly from the arterial limb with the help of a syringe and discarded. After that, the blood takes for the measurement of the post-dialytic urea value.
- Only then can the blood be returned.
Take Home Message
- Kt/V is the standard parameter for the removal of the small molecule like uremic toxins in hemodialysis
- Falling below a Kt/V value of 1.2 (corresponding to a URR of about 65%) correlates negatively with patient survival.
- The prescribed and actually administered dialysis dose differ mainly due to incorrect blood pump calibration, unnecessary blood flow reduction, e.g., in the case of hypotension, problems with vascular access, and arbitrary shortening of time due to patient intolerance or lack of patient compliance.
- It is therefore certainly a good idea to aim for a target Kt/V of 1.3 – 1.4 to truly achieve the minimum value of 1.2.
- Incorrect blood collection technique, particularly at the end of dialysis, is a major cause of incorrectly determining Kt/V values.
please can you explane me in easy word how find clearance k of dialyser
The urea clearance value (K) of all dialyzer types can be found in the product description.