Continuous Renal Replacement Therapy (CRRT)
Continuous renal replacement therapy (CRRT) means all extracorporeal dialysis and hemofiltration treatments that are usually carried out under intensive care conditions without significant interruption over 24 hours on one or more days and are primarily used in acute kidney failure.
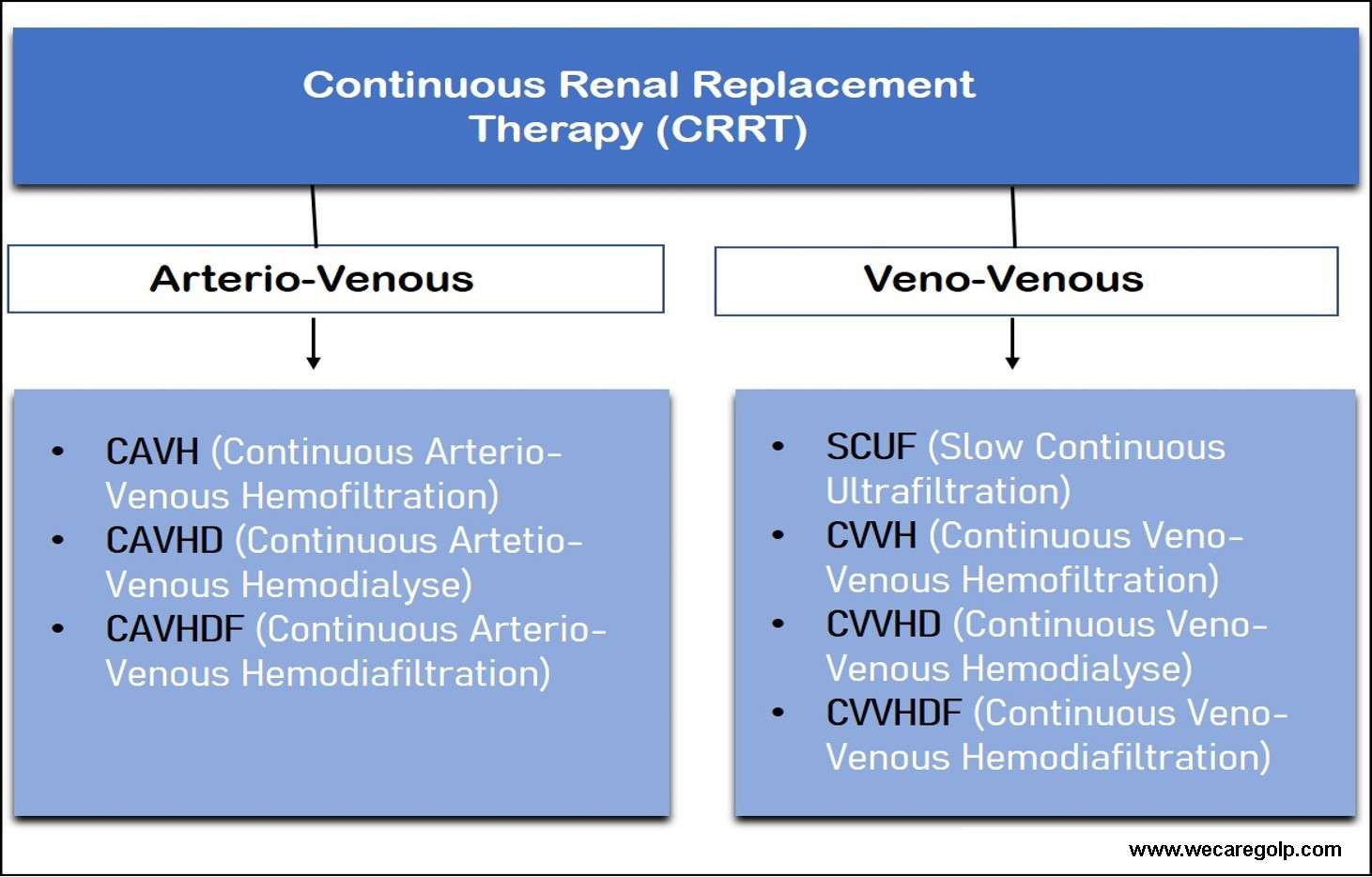
Types of Continuous Renal Replacement Therapy (CRRT)
Continuous Arterio-Venous Method
- The continuous arterio-venous method is the oldest and technically simplest process.
- It has different types like CAVH (Continuous Arterio-Venous Hemofiltration), CAVHD (Continuous Arterio-Venous Hemodialysis) and CAVHDF (Continuous Arterio-Venous Hemodiafiltration).
- The arterial blood pressure determines the blood flow and the amount of filtrate.
- This method will carry out without any technical equipment. However, an arterial (femoral artery) and a venous (femoral vein) catheter is made.
- Spontaneous filtration takes place.
- A small hemofilter is placed between the artery and vein using blood tubing connections.
- The treatment is no longer effective when systolic blood pressure is below 100 mmHg. Therefore, it can use to a limited extent in patients.
Continuous Veno-Venous Method
This method is a pump-assisted extracorporeal blood purification process.
1. SCUF (Slow Continuous Ultrafiltration)
- SCUF is the simplest continuous veno-venous method.
- It is slow, isolated ultrafiltration designed to correct the patient’s net fluid balance.
- In this procedure, the blood is usually taken from a double-lumen CVC (central venous catheter) with the help of a blood pump and passed through a hemofilter (high-flux filter) with a blood flow of 50 – 200 ml/min.
- On the filtrate side, a set amount of liquid is ultrafiltered with a UF pump. The UF measures in the empty bag of a balance or a volumetric chamber.
- In this system, only the patient’s net UF removes, and no substitution is connected.
- Therefore, the SCUF can indicate the condition of fluid overload due to kidney or heart failure (cardio-renal syndrome) with possible complications such as pulmonary or brain oedema.
- It can also use as a supportive therapy, eg. for parenteral nutrition and oligo-anuria.
- It is not sufficiently efficient like hemodialysis.
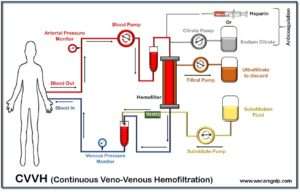
2. CVVH (Continuous Veno-Venous Hemofiltration)
- The CVVH is a classic hemofiltration method with low filtrate flow.
- In this method, double-lumen venous access is established in the femoral, jugular, or subclavian veins.
- It is thus possible to adapt both the blood flow and the filtrate and substitute flow to the therapy requirements independently of the patient’s blood pressure.
- In contrast to many hemofiltration devices, the CVVH machine offers the option of setting a low filtrate flow to carry out the slowest possible treatment.
- There are no major differences between a CVVH and a hemofiltration machine regarding the fluid balance and blood pump.
- The effectiveness of the CVVH depends exclusively on the filtration rate.
- As with all hemofiltration processes, the elimination of urinary substances takes place according to the principle of convection.
- A blood flow of 120-200 ml/min and a filtrate flow of 30-50 ml/min can recommend as standard settings.
- The CVVH can carry out over 24 hours a day. One advantage of the CVVH is the possibility of monitoring the extracorporeal circuit using the control and safety devices of the CVVH machine.
- In addition, the blood, filtrate and substitute flow can adjust depending on the blood pressure.
- The volume exchange can increase by increasing blood flow, filtrate and substitute rates up to 100 l / day.
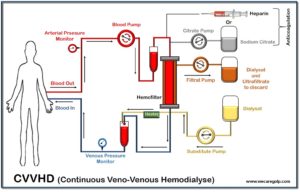
3. CVVHD (Continuous Veno-Venous Hemodialysis)
- The CVVHD is a pump-assisted extracorporeal blood purification process.
- Here is the diffusive transport system responsible for the elimination of urinary substances.
- This procedure will carry out with the same treatment machine-like CVVH.
- In contrast to the CVVH, the substitute and filtrate pumps require to generate a dialysate flow in the hemofilter.
- The substitute pump conveys the dialysis solution through the substitute system into the filter.
- As the dialysis solution can use either bicarbonate or lactate
- If the substitute pump and the filtrate pump run at the same speed, there is no ultrafiltration from the blood.
- For ultrafiltration, the filtrate pump must run faster than the substitute pump.
- The average blood flow for CVVHD should be 120-200 ml/min, and the dialysate flow should be 20-40 ml/min.
- The CVVHD can use when the continuous clearance of the CVVH in the small molecular range (e.g. urea, creatinine, potassium) is insufficient.
4. CVVHDF ((Continuous Veno-Venous Hemodiafiltration)
- CVVHDF combine the technical possibilities and advantages of hemodialysis and hemofiltration.
- The CVVHDF has the highest clearance rates of all continuous methods of renal replacement therapy.
- In practice, this method is currently rarely used. The reason for this probably lies in its complex extracorporeal system and the increased consumption of substitution solution, with the associated costs.
Indications of continuous renal replacement therapy
- Metabolic acidosis
- Volume overload
- Electrolyte abnormalities (hyponatremia, hyperkalaemia, hyperphosphatemia)
- Uremia
- Encephalopathy
- Pericarditis
- Persistent/progressive acute kidney injury
Complications of continuous renal replacement therapy
Technical Complications
- Filter closure
- Blood flow problem
- Disconnection / kinking of the hose line
- Fluid balance errors
Medical complications
- Hypotension
- Bleeding
- Thrombosis
- Infection / sepsis
- Hypothermia allergy
Advantages of CRRT
- Low expenditure on equipment for processes that are not supported by pumps.
- Constant volume and toxin withdrawal.
- Maintain acid-base balance constantly.
- Low blood pressure is rare.
Disadvantages of CRRT
- The procedures require the entire daily routine for application and can therefore only carry out on immobilized intensive care patients.
- Rapid correction of life-threatening electrolyte imbalances (acute hyperkalaemia) is not possible.
- An arterial and venous vascular access require for the non-pump-assisted procedures.
- Sufficiently high blood pressure needs for non-pump-assisted procedures. If the blood pressure is less than 70 mmHg, the blood flow and the filtration rate decrease. Sufficient clearance is therefore no longer guaranteed.
- The material costs are high.
- Continuous anticoagulation is essential.
References
- Continuous Renal Replacement Therapy (nih.gov)
- Continuous Renal Replacement Therapy (CRRT) | Asahi Kasei Medical Co., Ltd. (asahi-kasei.co.jp)
- Frontiers | Continuous Renal Replacement Therapy: A Review of Use and Application in Pediatric Hematopoietic Stem Cell Transplant Recipients | Oncology (frontiersin.org)
- Continuous renal replacement therapy: recent advances and future research | Nature Reviews Nephrology
1 thought on “Continuous Renal Replacement Therapy (CRRT)”