Introduction
An ABG (arterial blood gas) analysis is a blood test that measures the levels of arterial partial pressure of oxygen (PaO2), blood pH, and arterial partial pressure of carbon dioxide (PaCO2) in the blood. Usually, a blood sample is drawn from the vein but in this procedure, blood is drawn from the artery. There is a similar procedure called “blood gas analysis” in which blood samples can be obtained from anywhere in the circulatory system, e.g., capillaries, arteries, and veins.
The artery is a major part of the circulatory system which carries oxygenated blood away from the heart to other body parts. They do not contain valves and are not collapsible. Artery walls are stronger than veins.
Other names of ABG analysis are
- Blood gas test
- Blood gas analysis
- Arterial blood gases
- ABG
In addition to PaO2, PaCO2, and pH, it can also determine arterial oxygen saturation (SaO2), bicarbonate (HCO3), hemoglobin, several electrolytes, etc.
In general, ABG analysis gives the information on how well the kidneys and lungs are working to maintain acid-base balance. ABG is one of the most commonly used procedures in those settings which required prompt treatment. ICU and emergency ward are places where ABG test is done frequently but it can be done on any patient depending on their diagnosis. This procedure needs skill and trained personnel because blood drawn from arteries is much more painful than veins.
Purposes of ABG analysis
- To assess the presence of acidosis (<7.35) or alkalosis (>7.45)
- To determine how well the kidneys and lungs are working (measuring O2 and CO2 levels)
- To identify certain medical conditions like kidney diseases, lung diseases, metabolic diseases, etc.
- To calculate the serum anion gap.
- To identify the compensatory process and treat accordingly.
- To assess the response of therapy and therapeutic intervention (mechanical ventilator).
Components of ABG and its Parameters
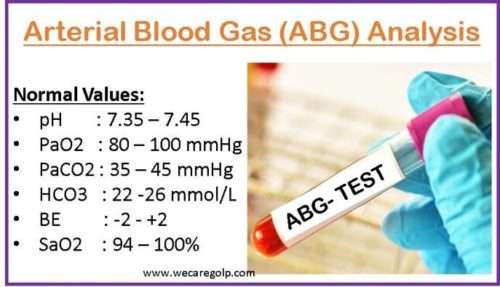
| S.N. | Components | Description | Normal Range |
| 1 | Power of hydrogen (pH) | Identifies the presence of acidemia or alkalemia in the blood | 7.40 (7.35-7.45) |
| 2 | Partial pressure of oxygen (PaO2) | Pressure exerted by oxygen dissolved in the blood | 80-100 mm Hg |
| 3 | Partial pressure of carbon dioxide (PaCO2) | Pressure of dissolved carbon dioxide in arterial blood | 35-45 mm Hg |
| 4 | Bicarbonate (HCO3) | A chemical that helps prevent the pH of blood from becoming too acidic or too basic | 22-26mEq/L /mmol/L |
| 5 | Base excess (BE) | Calculated relative excess or deficit of base in arterial blood | +2 – -2 |
| 6 | Saturation of oxygen (SaO2) | The amount of oxygen being carried by the hemoglobin in the red blood cells | 94 – 100% |
Indications of ABG analysis
- Acute respiratory distress syndrome (ARDS): A life-threatening condition resulting in hypoxemia (low level of O2 in the blood) due to lung injury, sepsis, respiratory diseases, and other conditions.
- Severe sepsis: A condition where the body’s response to infection involving multiple organ damage and widespread infection leads to a dysfunction of the respiratory and metabolic state of the body.
- Septic shock: A severe condition caused by any type of bacterial infection leading to a dangerously dropped in blood pressure.
- Hypovolemic shock: An emergency condition in which the heart is unable to pump enough blood due to excessive fluid or blood loss.
- Diabetic Ketoacidosis (DKA): A serious and life-threatening complication of diabetes (mainly Type 1 diabetes) and those who have undiagnosed Type 1 diabetes. In DKA, blood becomes more acidic.
- Renal tubular acidosis (RTA): A condition where kidneys are unable to remove acid causing blood to become acidic.
- Cardiac arrest: A condition in which the heartbeat stops suddenly.
- Acute respiratory failure: A condition of lungs and blood function alteration due to fluid building up in the alveoli, which makes it difficult to release oxygen from the lungs.
- Acute heart failure: A condition of sudden weakening of the heart that limits its function.
- Asthmatic attack: A condition of sudden worsening of asthma symptoms that is caused by the tightening of muscles around airways causing respiratory acidosis.
- Burn: Excessive burn causes metabolic acidosis which usually develops within 2 hours of burn injury.
- Poisoning: Mainly, it causes metabolic acidosis
Contraindications of ABG Sampling
- Local infections or cellulitis
- Arteriovenous fistula
- Distorted anatomy (unable to palpate pulse)
- Peripheral vascular diseases
- Coagulopathy known cases
- Arterial graft
- Absent collateral circulation
- Raynaud’s diseases
Site for Sampling
Mainly, blood for ABG analysis is drawn from the radial artery. Unfortunately, getting a sample from an artery is more painful than a vein because arteries are deeper than vein.
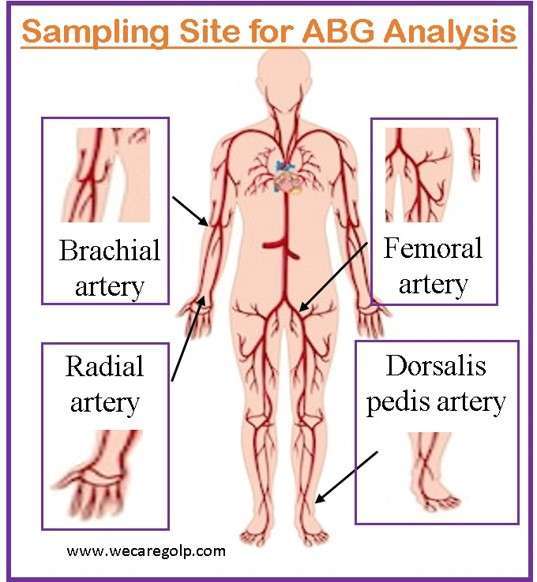
- The common site for sampling
- Radial artery: palmar crease area, between the radial styloid process and the flexor carpi radialis tendon (the nondominant limb is preferred).
- Alternative sites
- Brachial artery: in the elbow (this site is not recommended due to the risk of hematoma causing nerve compression; if used, the nondominant limb is preferred)
- Femoral artery: midline between the symphysis pubis and the anterior superior iliac crest
- Dorsalis pedis artery
- Posterior tibial artery (rarely used)
- In newborns
- Umbilical artery
Equipment Required for ABG Analysis
- Gloves
- Heparinized syringe (3cc or 1cc)
- Dry cotton
- Alcohol wipe or gel
- Tape
- Pillow or blanket to rest wrist during sampling
- A plastic bung
- Local anesthesia: 1% Lignocaine and syringe
- 23 G needle
- Patient label
Procedure of ABG Analysis
Before the Procedure
- Explain the procedure to patient and inform him/her that this procedure is painful.
- Take verbal consent from the patient.
- Collect articles to bedside.
- Place the patient in a comfortable position.
- Reassurance to patient.
During the Procedure
- Wash the hand properly.
- Wear gloves.
- Clean the selected site to be punctured with alcohol or a spirit swab.
- A pre-existing arterial line can be used to obtain the blood sample if the patient has already one.
- It is recommended that the Allen test (modified) should be performed before an arterial puncture and particularly before an arterial puncture on radial site.
- When the Allen test is positive, draw the sample in an aseptic technique from the selected site.
- With two fingertips hold the artery after pulsation is felt and then insert the heparinized needle at a 90˚ angle.
- After the insertion of the heparinized needle, blood outflow is observed and is conformed by withdrawing 1 ml of blood by gently pulling the syringe plunger.
- During the gently pulling of the plunger do not aspirate the air into the syringe. Because aspiration of air leads to air in the sample, leading to error.
- After sample collection, cover the needle or syringe with its cap.
- Apply compression to the punctured site until the bleeding stops.
- Label the sample with the information of the patient correctly.
Allen test
A medical procedure used to assess the patency of the arteries (radial and ulnar) in the hand is called the Allen test. It is usually done before arterial blood gas sampling to ensure adequate blood supply to the hand.
Procedure of allen test
- Ask the patient to make a fist to enhance the circulation within the hand.
- Feel the pulse on both the radial (thumb side) and ulnar arteries in the wrist, then compress both arteries simultaneously.
- The compression stops blood flow to the hand temporarily.
- Release the pressure on the ulnar artery while continuing to compress the radial artery, and at the same time, ask the patient to open the hand.
- The test is considered positive if the patient’s hand regains quickly (within 5 – 15 seconds) its color indicating that the open ulnar artery is providing sufficient blood flow.
- If the patient’s hand does not regain color or takes longer than 15 seconds to do so, it may indicate arterial occlusion or insufficiency. It could potentially be the contraindication for ABG sampling.

After the Procedure
- Remove gloves.
- Wash the hands.
- Put the patient in a comfortable position.
- Replace articles or proper disposal of the used articles.
- Assess the punctured site for bleeding or hematoma.
- Once the arterial blood sample is obtained, it is sent to the lab for analysis. Usually, most emergency and intensive care units have one blood gas analyzer for quick results.

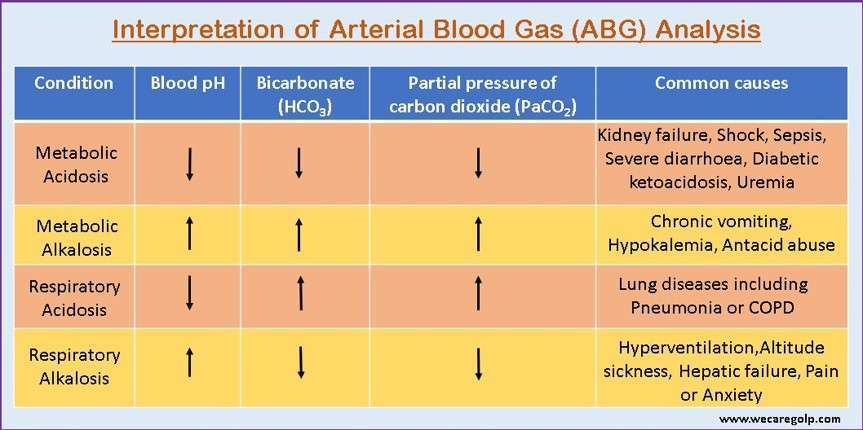
Interpretation of ABG Analysis
Analysis of arterial blood gases helps us to know whether the patient’s condition is severe or not. With the help of this analysis, the different types of acid-base imbalances can be ruled out so that the patient gets better treatment.
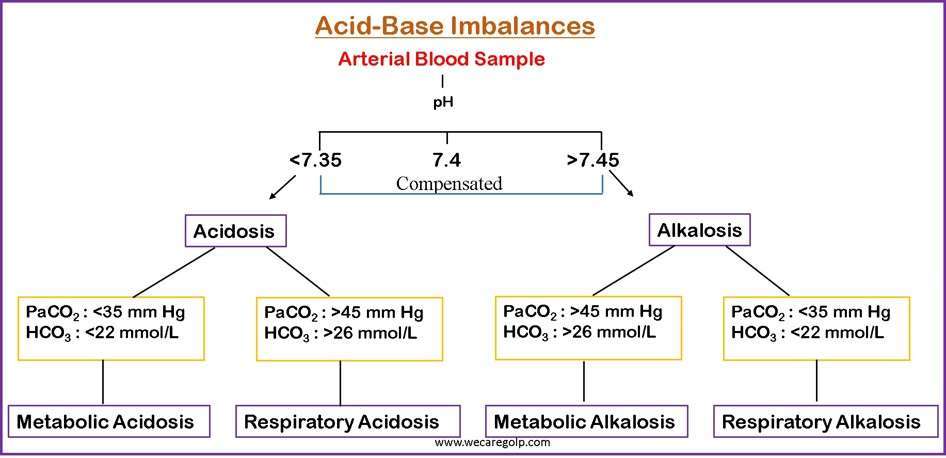
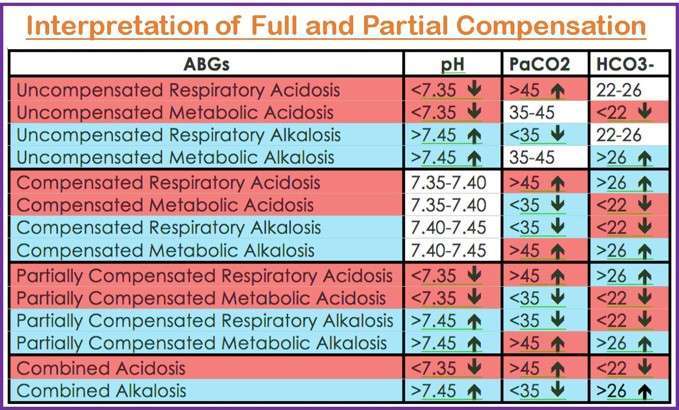
- Step 1: Firstly, look at the pH to determine the presence of acidosis (pH <7.35) or alkalosis (pH >7.45).
- Acidosis or alkalosis may still be present even if the pH value is in the normal range, as the body can compensate to balance the pH.
- Remember, the lower the pH number, the higher the acid level in the body.
- Step 2: Evaluate the disturbances, whether it is respiratory or metabolic. Here, the PaCO2 in combination with HCO3 determines the types of acid-base imbalances.
- Remember, when the pH and PaCO2 change in the opposite direction, it indicates primary respiratory disorders.
- On the other hand, if pH and PaCO2 change in the same direction, it indicates metabolic disorders. The chart below explains more.
- Step 3: Identify if there is appropriate compensation for the primary disturbances.
- Full compensation if the pH is within the normal range
- Partial compensation if all three (pH, PaCO2, and HCO3) values are out of range
The following chart helps to illustrate the compensation
- Step 4: Lastly, assess the PaO2 for any abnormalities in oxygenation.
Complications of During and After ABG Sampling
Minor complications
- Bleeding
- Pain and Infection at the punctured site
- Feeling faint or dizziness
- Hematoma
- Numbness of hand
Major complications
- Thrombosis
- Major hematoma or hemorrhage
- Pseudo aneurysms
- Nerve damage
- Arterial occlusion
Summary
- Arterial blood gas (ABG) analysis is a medical procedure that measures the oxygen, carbon dioxide, and acidity (pH) levels in the arterial blood.
- It is usually performed in emergency and critical care units to assess and monitor acid-base balance and function of the lungs.
- It provides important information about the respiratory and metabolic status of the patient.
- A blood sample is drawn from an artery (typically from the radial artery) during an ABG analysis.
- The main parameters measured in an ABG analysis include pH, PaO2, PaCO2, HCO3, and SaO2.
- It helps diagnose various conditions such as respiratory disorders (e.g., asthma, chronic obstructive pulmonary disease), and metabolic disorders (e.g., diabetic ketoacidosis), and assess the effectiveness of respiratory interventions and treatments.
References
- Arterial Blood Gases (ABGs) Explained. nurse.org. Retrieved on 2023, May 12 from https://nurse.org/articles/arterial-blood-gas-test
- Castro, D., Patil, S.M., Keenaghan, M. (2022, Sep 12). Arterial Blood Gas. StatPearls Publishing. Retrieve on 2023, May 13 from https://www.ncbi.nlm.nih.gov/books/NBK536919/
- Gaines, k. (2023, April 26). Arterial Blood Gases (ABGs) Explained. nurse.org. Retrieved on 2023, May 12 from https://nurse.org/articles/arterial-blood-gas-test
- World Health Organization. (2010). Modified Allen Test. Retrieved on 2023, May 12 from www.ncbi.nlm.nih.gov/books/NBK138652
- Rose, B.D. and Post, T.W. (2001). Clinical physiology of acid-base and electrolyte disorders. New York: McGraw Hill Medical Publishing Division, 2001, 5th edition.